Transmasculine Guide: Dosing
Dosing (gels):
Section titled “Dosing (gels):”Here is a table of typical doses of testosterone gel used in transmasculine hormone therapy:
| Testosterone Gel Type | Low Dose | Initial - Typical Dose | Maximum - Full Dose | Additional Notes |
|---|---|---|---|---|
| Testosterone topical gel 1% (packet) | 12.5-25 mg daily | 50mg daily | 100mg daily | Usually comes in packet form |
| Testosterone topical gel 1.62% (packet or pump) | 20.25mg daily | 40.5 - 60.75mg daily | 103.25mg daily | Comes in either packet/pump form. One packet/pump = 20.25mg |
| Testosterone axillary gel 2% (pump bottle) | 30mg daily | 60mg daily | 90-120mg daily | Comes in pump form only, one pump = 30mg |
It is recommended that people start on ~50mg of testosterone gel per day, up to a maximum of 100mg/day.
Testosterone gel can be applied to the shoulders and upper arms, or the stomach area. Thoroughly rub in the gel, and wait until it is completely dry before putting on clothing or interacting with pets.
It is not recommended you go over 100mg/day unless you have obvious signs of insufficient T levels after a year on that dosage (still having menstrual cycles, or a blood test showing inadequate levels).
Keep in mind the low dosage range described above will generally not induce the same extent nor speed of changes as what would be expected at higher dosages.
Calculating Gel Dosages
Section titled “Calculating Gel Dosages”Gel that comes in a pump style bottle will usually say exactly how much testosterone will be dispensed per pump (usually 20.25mg or 30mg).
With individual gel packets, some products clearly state on the box or packet how much testosterone each packet contains. However, some brands do not list this directly, so a simple calculation may be necessary. Gel packets usually provide the concentration as a percentage (commonly 1%) and the total amount of gel in the packet (typically 2.5 grams or 5 grams).
To calculate the amount of testosterone in a packet, use the following formula:
(gel packet volume in grams) × (concentration of gel as %) × 100 = amount of testosterone contained in each packet
Dosing examples (Includes some common formulations):
Section titled “Dosing examples (Includes some common formulations):”| Gel packet volume in grams | Concentration of gel as % | Calculation | Amount of testosterone contained in each packet |
|---|---|---|---|
| 1.25g | 1.62% | 1.25 × 1.62 × 100 = 20.25 | 20.25mg |
| 2.5g | 1% | 2.5 × 1 × 100 = 25 | 25mg |
| 5g | 1% | 5 × 1 × 100 = 50 | 50mg |
Not too complicated now, hopefully!
Dosing (injections):
Section titled “Dosing (injections):”Here is a table of typical doses of injectable testosterone used in transmasculine hormone therapy:
| Type | Low Dose | Initial - Typical Dose | Maximum - Full Dose |
|---|---|---|---|
| Testosterone Cypionate | 20 mg/week | 50 mg/week | 100 mg/week |
| Testosterone Enanthate | 20 mg/week | 50 mg/week | 100 mg/week |
You can either choose to slowly ramp up your dosage, or you can start at a full dose. Neither method is necessarily better than the other.
It would not be recommend you go over 100mg/week unless you have obvious signs of insufficient T levels after a year on that dosage (still having menstrual cycles, or a blood test showing inadequate levels). It is still highly recommended you get blood testing though, as having very high T levels can increase polycythemia risks.
Keep in mind the low dosage range described above will generally not induce the same extent nor speed of changes as what would be expected at higher dosages.
Dosing (testosterone undecanoate):
Section titled “Dosing (testosterone undecanoate):”| Type | Low Dose | Initial - Typical Dose | Maximum - Full Dose |
|---|---|---|---|
| Testosterone Undecanoate in castor or grapeseed oil (ie. Nebido or anything pharmacy sourced) | 80mg every month (every 28-31 days) | 200mg every month (every 28-31 days) | 400mg every month (every 28-31 days) |
| Testosterone Undecanoate in MCT oil (will usually be from steroid sellers) | 60mg every 3 weeks (21 days) | 150mg every 3 weeks (21 days) | 300mg every 3 weeks (21 days) |
With long acting esters like testosterone undecanoate, the carrier oil can affect how long it stays in the body, which is why dosing may vary by formulation.
It can also be hard to source and is often only available in single use ampules rather than multi dose vials. These typically contain 1000 mg, which is usually too high, leading to excessive levels and large fluctuations. They also require injecting about 4 mL, which can be painful. For these reasons, ampules are not recommended, and vials are preferred instead.
Keep in mind the low dosage range described above will generally not induce the same extent nor speed of changes as what would be expected at higher dosages.
Because testosterone undecanoate builds up slowly, an initial loading dose of up to 2.5× your regular dose can be used to reach stable levels faster. For example, if your intended dose is 300 mg every three weeks, your initial loading dose may be 600 mg (300 × 2.5).
Calculating Injection Dosages
Section titled “Calculating Injection Dosages”Vials of testosterone are usually compounded at either 200mg/mL, 250mg/mL or 300mg/mL. This means that for a 200mg/mL vial, every 1mL of liquid will contain 200mg of testosterone. A 10mL vial will then contain a total of 2000mg of testosterone. Keep in mind that higher concentrations of T may cause more post-injection pain, due to higher ratio of solvent used in the vials.
We will unfortunately be doing some math here.
The formula to calculate how much liquid to inject is:
(amount you want to inject) ÷ (concentration of the vial) = amount to inject per dose in mL
Dosing examples:
Section titled “Dosing examples:”| Desired Dose | Vial Concentration | Calculation | Injection Volume |
|---|---|---|---|
| 20mg | 200mg/mL | 20 ÷ 200 = 0.1 | 0.1mL |
| 50mg | 200mg/mL | 50 ÷ 200 = 0.25 | 0.25mL |
| 100mg | 200mg/mL | 100 ÷ 200 = 0.5 | 0.5mL |
| 50mg | 250mg/mL | 50 ÷ 250 = 0.2 | 0.2mL |
| 50mg | 300mg/mL | 50 ÷ 300 ≈ 0.17 | 0.17mL |
Not too complicated now, hopefully! If you still need help with calculating dosages, This is a useful tool. It’s intended for transfems but is equally usuable for calculating testosterone vial dosages.
How to perform a T injection
Section titled “How to perform a T injection”Needles can be bought from any pharmacy over the counter in most countries without a prescription (you may have to ask the pharmacist directly). Most countries also have online sites that sell appropriate injection needles. Amazon is a popular source for those in America.
Injection Supplies
Make sure to buy 1mL syringes, as the small amounts of fluid we are using for each injection are only easily measured with 1mL syringes. The more common 3mL syringes will still work if you cannot find 1mL syringes, but are not ideal. It is fine to use 3mL syringes if you are using testosterone undecanoate due to the high injection volumes.
There are two methods for a T injection, subcutaneous/subq³ (injection into the layer of fat under the skin), and intramuscular/IM (injection deep into the muscle underneath the skin and fat). Both methods result in identical absorption rates and levels of the drug, whether you prefer subq or IM is mostly personal preference.
Homebrewed injections typically contain benzyl benzoate (a safe solvent that is also commonly used in prescription grade medications), which can cause some minor irritation if injected subcuaneously. Usually there will be less post-injection pain if injected intramuscularly.
Appropriate gauges (needle thickness) for a subcutaneous injection are 25-30g, for intramuscular, 23-25g. Subq needles are thinner than IM needles, which some people will find less intimidating.
Recommended needle lengths are as follows: 1”-1 ½” (IM, 1 inch is better for thinner people and 1 ½” for thicker people) ½”-⅝” (Subq, up to personal preference)
There are many online videos and guides for how to administer an intramuscular or subcutaneous injection, here is a decent one:
- Guide by Plume: https://support.getplume.co/support/solutions/articles/72000544742-all-about-injections Very detailed video guides on both IM and subq injections, with the downside that they are split into multiple long videos.
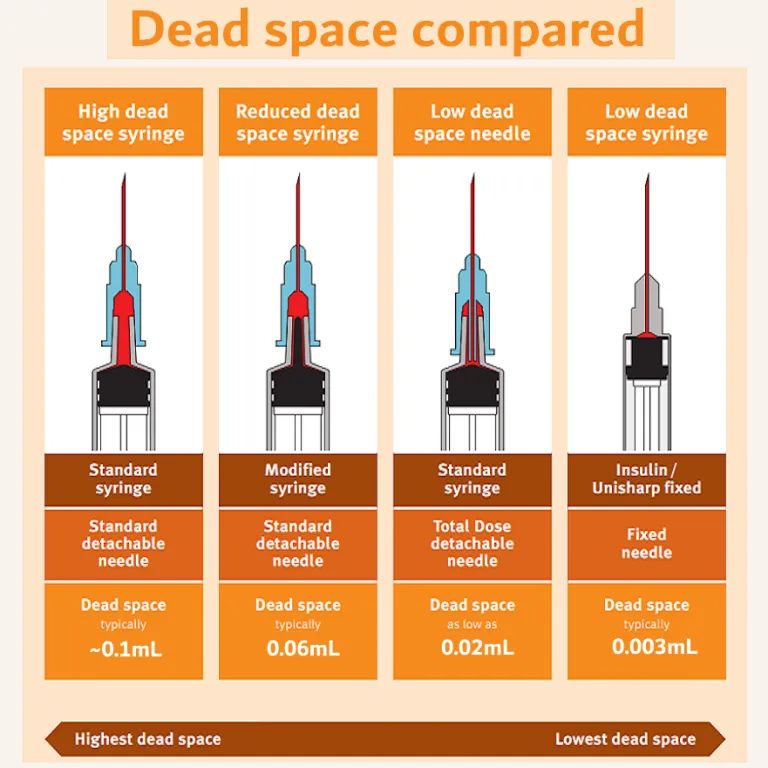
Note that around 0.1mL of fluid will be lost with each injection due to needle dead space.
Note on finasteride and dutasteride usage
Section titled “Note on finasteride and dutasteride usage”Some trans masculine people choose to take medications like finasteride or dutasteride to prevent male pattern baldness and hair loss.
These medications work by preventing testosterone from naturally converting into another hormone called DHT (dihydrotestosterone). DHT is the main hormone responsible for male pattern hair loss.
DHT also plays an important role in developing body and facial hair growth and bottom growth. If these changes are desired, it may be recommended to not take finasteride or dutasteride until you are satisfied with your level of facial and body hair growth and bottom growth. If finasteride or dutasteride is started too soon, these changes may be limited (though these changes will continue without issue if finasteride or dutasteride is stopped).
Male pattern hair loss is generally very rare in the first year of T, though if you are still concerned, minoxidil (brand name Rogaine) can be used as a topical hair loss prevention medication, and will not inhibit other desired changes.
Blood testing:
Section titled “Blood testing:”It is recommended to do your first blood test within the first 3 months, and then adjust your dosage if necessary. If you change your dosage, try to retest again within 3 months. If your levels look good, blood testing frequency can be reduced to just once a year.
Check out our blood testing page for sources near you:
Blood Test Sources
Get your estradiol (E2), total testosterone (T) and complete blood count (CBC) (also referred to as full blood count/FBC) tested every time. Get your blood taken as close as possible to your next scheduled injection/dose (Test your blood as far away as possible from a previous dose, right before your next scheduled dose. Preferably the day of your shot, or the day before).
Your blood levels of estradiol and testosterone when taken at this time are called ‘trough levels’, because they are the levels of E2 and T that are present in your body at the lowest point in your HRT dosing regimen.
What should my total testosterone (T) reading be?
The Endocrine Society’s 2017 clinical guidelines for transgender HRT recommend that trans men maintain “testosterone levels in the physiologic normal male range”, a range which is typically given as 300–1000 ng/dL. Slightly higher or lower testosterone levels above or below this range are not something to worry about unless your estradiol levels are also too high.
What should my estradiol (E2) reading be?
The typical range for adult males is 10 – 50 pg/ml although this varies due to age and individual factors. Try to aim within this range, although slightly higher levels are not something to worry about. Try to keep your estradiol under 70pg/mL.
What should my CBC look like?
Polycythemia is defined as serum hematocrit (Hct) or hemoglobin (HgB) exceeding normal ranges expected for age and sex, typically Hct > 49% in healthy adult males. So there no concern if you have Hct levels lower than that. If your levels are elevated, donating blood or reducing testosterone dose can treat polycythemia.
If your red blood cell (RBC) and hematocrit are above reference ranges on your CBC test, you may be at elevated thrombosis (blood clot) risk. You can donate blood or lower your dose to reduce this risk.
Donating blood is also a way to get your CBC checked for free, as CBC is typically checked every time someone donates blood.
Occasional Liver Function Tests (LFT)/Liver enzymes, Clotting factors test, and Lipid profile test (cholesterol, triglycerides) can be useful to monitor certain health risks associated with testosterone therapy. Though these risks would usually only be relevant at excessively high dosages.
Hormone therapy in general is very safe and effective as long as you take reasonable doses.